This indicator provides an overview of system-wide radiotherapy activity in Australia, as provided through the Medicare Benefits Schedule (MBS). For the purposes of these analyses, cancer related treatments include “key selected radiotherapy procedures performed with the general intent to change the outcome of the cancer and/ or provide symptom relief/palliative care”. There are two main modes of radiotherapy delivery for the treatment of cancer – internal and external beam radiotherapy1:
Internal/ systemic radiotherapy
- Internal radiotherapy involves delivery of radiation via a needle, catheter or another specialised device. Delivery may be via two mechanisms:
- Implantation of sealed radioactive sources inside the body into or near the tumour (also called brachytherapy).
- Delivery of liquid radioisotopes (radioactive drugs) given by mouth or put into a vein (intravenous delivery), these drugs then travel throughout the body.
External beam radiotherapy
- External beam radiotherapy (called external beam radiation) uses a machine to beam radiation (x-rays or gamma rays) at the tumour.1 The area that receives radiation is very precise, minimising the amount of radiation on surrounding healthy areas. It is used in the treatment of a wide range of cancer types including breast, lung, prostate and gynaecological cancers.2
- External beam radiotherapy delivery can be broadly grouped into 3 categories, primarily based on the depth of penetration of the radiation:
- Superficial radiotherapy utilises low energy ionizing radiation to treat cancer and other conditions that occur either on, or close to the skin surface.
- LINAC radiotherapy using a machine called a linear accelerator (also called a LINAC), which uses electricity to create high-energy radiation for treatment of tumours deep within the body.
- Other types of external beam radiotherapy - including deep or orthovoltage radiotherapy, cobalt/caesium radiotherapy and stereotactic radiotherapy.
More than 99% of radiotherapy services billed to the MBS are external beam radiotherapy (refer diagram A), and almost 97% of these are performed using a linear accelerator (LINAC; refer diagram B). This indicator of radiotherapy activity therefore primarily focuses on LINAC radiotherapy treatment activity.
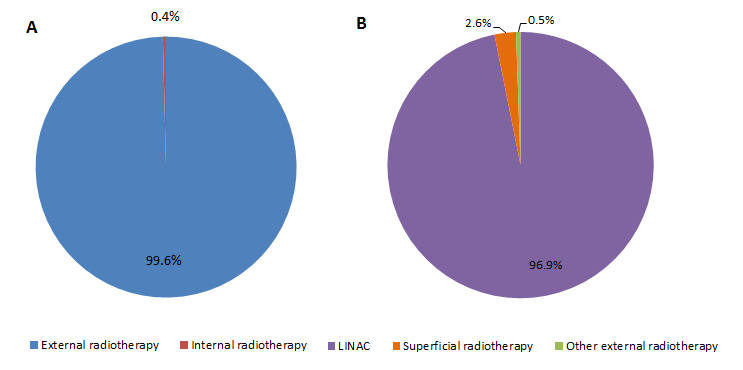
*Example data shown are for 2013. Brachytherapy is often administered on an admitted patient basis and may not be included in MBS data.
Specific information about data sources, and guidance for interpreting the data, can be found in the ‘About the Data’ tab and definitions of key terms are provided in the ‘Glossary’ page.
About this measure
The measure "Radiotherapy treatment activity" presents data for radiotherapy services delivered in Australia between 2013 and 2015, as indicated by reimbursement claims under the Medicare Benefits Schedule (MBS). Some services are not eligible for reimbursement under the MBS, therefore these data would provide underestimates of the actual number of services being provided. The MBS data does not include detailed information on cancer types, therefore the services data presented are for the treatment of “all cancers combined”.
This analysis focusses primarily on external beam radiotherapy. The categories used for external beam and internal radiotherapy are provided in Table 1. Refer to ‘About the data’ for the definition and the MBS item codes used to define radiotherapy categories.
Table 1. Radiotherapy procedure categories
| External radiotherapy | Internal radiotherapy |
Categories used in this analysis | LINAC | Radioactive sealed sources |
Superficial radiotherapy | Radioisotope delivery | |
Other external radiotherapy* |
*Other external beam radiotherapy comprises deep or orthovoltage radiotherapy, cobalt/caesium teletherapy unit and stereotactic radiotherapy. See ‘About the data’ for definitions.
Trends
During the period 2013 to 2015
All LINAC services:
- The number of LINAC services provided (as indicated through MBS reimbursement claims) increased annually between 2013 and 2015.
- The number of services increased overall by 15% (from 1,002,047 to 1,062,702) between 2013 and 2015.
Age and Sex:
During the period 2013 to 2015, the proportion of services provided related to age group and sex varied:
- The proportion of annual separations was consistently higher for males (50-51% of services) than females (49-50%).
- Between 2013 and 2015, the number of LINAC services increased overall by around 6% for both sexes (females from 490,054 to 521,652 services and for males from 511,993 to 541,050).
- The highest proportion of separations by age was for the age group 65−74 years, accounting for 31-32% of annual services.
For females:
- The age group which accounted for the largest proportion of services varied over time:
- In 2013, females aged 55-64 years accounted for the largest proportion of services (27%; 133,967 services).
- In 2015, the 55-64 years and 65-74 years age groups each accounted for 27% of services (139,306 and 139,994 services, respectively).
- Females aged 55 years and older accounted for about two-thirds of LINAC services accessed by females. This proportion increased over time from 67% (327,692 services) to 69% (358,373 services) for this age group between 2013 and 2015, respectively.
For males:
- The age group which accounted for the largest proportion of services remained consistent:
- In 2013, the age range 65−74 years accounted for over a third of the male population who used these services (36%; 185,915 services).
- In 2015, this age-group accounted for a similar proportion of services (37%; 200,477 services).
- Males aged 55 years and older accounted for most of the LINAC services accessed by males. The proportion remained relatively consistent over time from 86% (440,752 services) to 88% (473,850) for this age group in 2013 and 2015, respectively.
Remoteness area of residence:
During the period 2013 to 2015, the distribution of LINAC services by remoteness area of residence remained relatively consistent:
- The majority of LINAC services provided were for people living in Major Cities; with 670,024 services (67%) and 706,399 services (66%) in 2013 and 2015, respectively.
- Around one third of services were for people living in Inner/Outer regional areas (between 31-32% annually), with 313,285 (31%) and 340,702 (32%) services in 2013 and 2015, respectively.
- Around 1.5% of the services provided were for people living in Remote/Very Remote areas; with 14,760 and 15,601 services (both 1.5%) in 2013 and 2015, respectively.
This indicator measures the number of radiotherapy services provided. Using the available data, it is not possible determine the number of individual patients accessing these services. As individuals may have multiple claimable services, which can also vary for different cancer types throughout a single course of radiotherapy treatment, comparison of the remoteness distribution of the number of LINAC services provided with incidence of all cancers is not considered to be appropriate. Direct comparison of these figures to the incidence of all cancers combined by remoteness area would be potentially misleading and as such has not been undertaken.
Socioeconomic status:
During the period 2013 to 2015, the distribution of LINAC services related to socioeconomic status areas has remained relatively consistent:
For females:
- About 26% of annual LINAC services for females were for those living in the highest SES areas (SES5) across this time period (from 129,024 to 138,014 services in 2013 and 2015 respectively).
- Approximately 15% of all annual LINAC services for females were for those living in the lowest SES areas (SES1) across this time period (from 73,454 to 79,180 services in 2013 and 2015 respectively).
- The proportion of annual LINAC services for females was similar for the other SES areas (SES 2-4), with 19-21% of services for each group.
For males:
- Between 22-23% of annual LINAC services for males were for those living in the highest SES areas (SES 5) across this time period (from 114,374 to 121,049 services in 2013 and 2015 respectively).
- Approximately 17% of annual LINAC services for males were for those living in the lowest SES areas (SES1), across this time period (from 84,656 to 92,368 services in 2013 and 2015, respectively).
- The proportion of annual LINAC services for males was similar for the other SES areas (SES 2-4), with 20-21% of services for each group.
This indicator measures the number of radiotherapy services provided. Using the available data, it is not possible determine the number of individual patients accessing these services. As individuals may have multiple claimable services, which can also vary for different cancer types throughout a single course of radiotherapy treatment, comparison of the socioeconomic status areas distribution of the number of LINAC services provided with incidence of all cancers is not considered to be appropriate. Direct comparison of these figures to the incidence of all cancers combined by remoteness area would be potentially misleading and as such has not been undertaken.
About the data
This measure shows the number of radiotherapy services processed by Medicare Australia over time and by population group.
Unit of analysis:
The MBS data summarised here outlines the number of radiotherapy “services” for which a reimbursement is claimed under the Medicare Benefits Schedule and processed by Department of Human Services. These types of data will allow for linkage of cancer incidence and radiotherapy services provided in later phases of STaR analyses and reporting.
Note: An additional source of data regarding radiotherapy treatment in Australia is the National Radiotherapy Waiting Times Database (NRWTD). Data are provided to the AIHW from jurisdictional health authorities and private radiotherapy providers. The unit of measure for the NRWTD data is the number of radiotherapy “courses” which is defined as a “series of one or more external beam radiotherapy treatments”3. (More information about the NRWTD can be found under the ‘References’ tab).
These datasets have a different scope and units of measure, and are therefore not directly comparable.
Scope:
The key radiotherapy services were chosen through a process of stakeholder consultation. The scope of the analysis is to provide an overview of system-wide radiotherapy activity in Australia, as provided through the Medicare Benefits Schedule (MBS). The MBS data does not include detailed information on cancer type; therefore the services data presented are for the treatment of “all cancers combined”.
For the purposes of these analyses, cancer related treatments include “key selected radiotherapy procedures performed with the general intent to change the outcome of the cancer and/ or provide symptom relief/palliative care”. Additional radiotherapy services such as planning and treatment verification services are not included.
In 2014, the scope of Medicare-subsidised radiotherapy services delivered overall (including planning and treatment verification services) was reported to be about 1.8 million (representing around 60,398 people)8. A similar figure of 1.9 million radiotherapy services was also reported for 2014-15.9
A more definitive national picture of radiotherapy activity for different cancers requires linkage to cancer incidence data. This will be investigated in future reporting through the STaR project.
Exclusions:
The MBS statistics do not include the following4:
- Services that are free-of-charge to patients in hospitals (i.e. services provided by hospital doctors to public patients in a public hospital)
- Services provided to the Department of Veterans’ Affairs beneficiaries
- Services that are the subject of compensation payments
- Health screening services
- Services conducted through State and Territory community controlled health centres.
Data source:
The data presented in this indicator are based on administrative information related to services that qualified for a Medicare benefit under the Health Insurance Act 1973 and for which a claim has been processed by the Department of Human Services between 1 January 2009 and 31 December 2015. Each MBS item code is associated with a claim, resulting in the payment of a Medicare Benefit being counted as a service.
Procedures:
In this indicator, the procedure codes as defined by the MBS have been classified according to the type of delivery (external and internal). Table 2 below comprises definitions of the categories reported and the corresponding MBS item codes. For a detailed description of the individual MBS item code, see www.mbsonline.gov.au.
Data caveats:
- Year is determined by the date the service was processed by Medicare Australia, not the date the service was provided.
- Figures are presented as aggregated frequency counts of services delivered in a single year rather than individual patients treated. Individuals may be counted more than once since they can have multiple claimable services throughout a single course of radiotherapy treatment.
- Information on cancer diagnosis cannot be reliably ascertained without using data linkage methods to combine information from multiple different data sources that is related to a single person.
- Radiotherapy can also be accessed through other arrangements which may not be covered by MBS. As a result, the number of MBS radiotherapy service counts may be an underestimate of the actual number of services.
Table 2. Definition of main categories and associated MBS item codes4
| Main category | MBS item codes |
|---|---|---|
External beam Radiotherapy | LINAC (Linear Accelerator) | 15215 15218 15221 15224 15227 15230 15233 15236 15239 15242 15245 15248 15251 15254 15257 15260 15263 15266 15269 15272 |
Radiotherapy superficial | 15000 15003 15006 15009 15012 | |
Other external beam radiotherapy (comprises deep or orthovoltage radiotherapy, colbalt/caesium teletherapy unit and stereotactic radiotherapy) | 15100 15103 15106 15109 15112 15115 15211 15214 15600 | |
Internal Radiotherapy | Radioactive sealed sources radiotherapy | 15303 15304 15307 15308 15311 15312 15315 15316 15319 15320 15323 15324 15327 15328 15331 15332 15335 15336 15338 15360 |
Radioisotope delivery | 16003 16006 16012 16015 16018 35404 35406 35408 (Excludes 16009) |
References
Activity in this area
Data:
Access MBS Patient Demographics data via:
Australian Institute of Health and Welfare 2017. Cancer in Australia 2017. Cancer series no. 101. Cat. no. CAN 100. Canberra: AIHW.
Australian Institute of Health and Welfare 2016. Radiotherapy in Australia: report on the second year of a pilot collection 2014–15. Cat. no. HSE 181. Canberra: AIHW. http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129557393
Barton MB, Jacob S, Shafiq J, Wong K, Thompson SR, Hanna TP, et al. Estimating the demand for radiotherapy from the evidence: a review of changes from 2003 to 2012. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2014;112(1):140-4. Epub 2014/05/17.7
Policy:
Department of Health. 2016. Medicare Benefits Schedule Review. Health: Canberra. http://www.health.gov.au/internet/main/publishing.nsf/content/mbsreviewtaskforce
References
1. Cancer Australia. Radiation therapy. Sydney: Cancer Australia; 2017 [Accessed January 2017]; Available at: https://canceraustralia.gov.au/affected-cancer/treatment/radiation-therapy.
2. Cancer Council NSW. Radiation therapy. Woolloomooloo: Cancer Council NSW; 2021 [Accessed January 2022]; Available at: https://www.cancercouncil.com.au/cancer-information/cancer-treatment/radiation-therapy/
3. Australian Institute of Health and Welfare 2016. Radiotherapy in Australia: report on the second year of a pilot collection 2014–15. Cat. no. HSE 181. Canberra: AIHW.
4. Department of Health. Medicare Benefits Schedule Data. Canberra: Department of Health; 2016 [Accessed January 2017]; Available at: http://www.health.gov.au/internet/main/publishing.nsf/Content/PHN-MBS_Data.
5. National Cancer Institute. Radiation Therapy for Cancer. Bethesda: NCI; 2017 [Accessed January 2017]; Available at: https://www.cancer.gov/about-cancer/treatment/types
6. Radiation Oncology Tripartite Committee. Planning for the Best: Tripartite National Strategic Plan for Radiation Oncology 2012-2022, version 1 Mount Druitt: 2012.
7. Barton MB, Jacob S, Shafiq J, Wong K, Thompson SR, Hanna TP, et al. Estimating the demand for radiotherapy from the evidence: a review of changes from 2003 to 2012. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2014;112(1):140-4. Epub 2014/05/17
8. Australian Institute of Health and Welfare 2017. Cancer in Australia 2017. Cancer series no.101. Cat. no. CAN 100. Canberra: AIHW.
9. Radiation Oncology: 2016 Review of the Radiation Oncology Health Program Grants (ROHPG) Scheme (http://www.mbsonline.gov.au/internet/mbsonline/publishing.nsf/Content/11B9EA8ED9992FE8CA257F4E001A413E/$File/2016%20ROHPG%20Review.pdf) [Accessed September 2017].